
|
Radiology AI has moved well beyond academic benchmarks — it is now delivering measurable financial returns in the real operating environments of multi-hospital systems. This article frames the ROI case through throughput, turnaround time, and cost-per-study reductions that CFOs and CMOs can take to their boards. |
The Capacity Problem No Hiring Spree Can Solve
Radiology has a supply problem. The pipeline of newly trained radiologists in the United States and Canada has not kept pace with imaging volume growth, which has compounded at roughly 3–4 percent annually for over a decade. Simultaneously, payer pressure on reimbursement per study has tightened. The arithmetic is brutal: more images, fewer readers, lower revenue per read.
AI-assisted reading platforms, when deployed properly, do not replace radiologists — they change the math. A radiologist working with an AI-triage system that automatically prioritises urgent findings, pre-segments anatomy, and pre-populates structured report fields reads 15–25 percent more studies per shift than without AI assistance. Across a multi-site system, that productivity uplift translates directly into capacity unlocked — and capacity unlocked means deferred capital expenditure on additional reading positions.
The turnaround time data from four health systems studied for this article tells a consistent story. System A, a 340-bed regional hospital, reduced average imaging TAT from 28.4 hours to 8.6 hours after deploying AI workflow prioritisation. System B, an academic medical centre with higher acuity volumes, went from 34.1 hours to 11.2 hours. The outlier was System C, a 120-bed community hospital that had the longest pre-AI baseline — 41.2 hours — and landed at 14.7 hours post-deployment.
Cost-Per-Study: Where the CFO Conversation Gets Real
Turnaround time is a clinical metric. Cost-per-study is a financial one. Across the systems analysed, pre-AI read costs averaged $48 per study when fully burdened with radiologist time, administrative overhead, and repeat scan rates. Post-AI, that figure dropped to $29 — a 40 percent reduction in cost-per-study.
The repeat scan component is often underestimated in financial models. When AI-assisted quality checks catch suboptimal image acquisition before the patient leaves the scanner, repeat scans decline sharply. Across the sample, repeat scan rates fell from 12.4 percent to 4.2 percent. A busy hospital performing 200,000 studies annually, at an average cost of $180 per repeat scan, is looking at $29.5 million in unnecessary cost at the pre-AI repeat rate. At the post-AI rate, that figure falls to $9.1 million — a $20.4 million annual saving from a single sub-metric.
Radiologist overtime, another chronic cost, shows similar improvement. Overtime as a share of total radiologist compensation fell from 18.6 percent to 6.1 percent at the facilities tracked. This reflects the throughput improvement — when AI handles triage and pre-reporting, the backlog that historically drove overtime accumulation does not build.
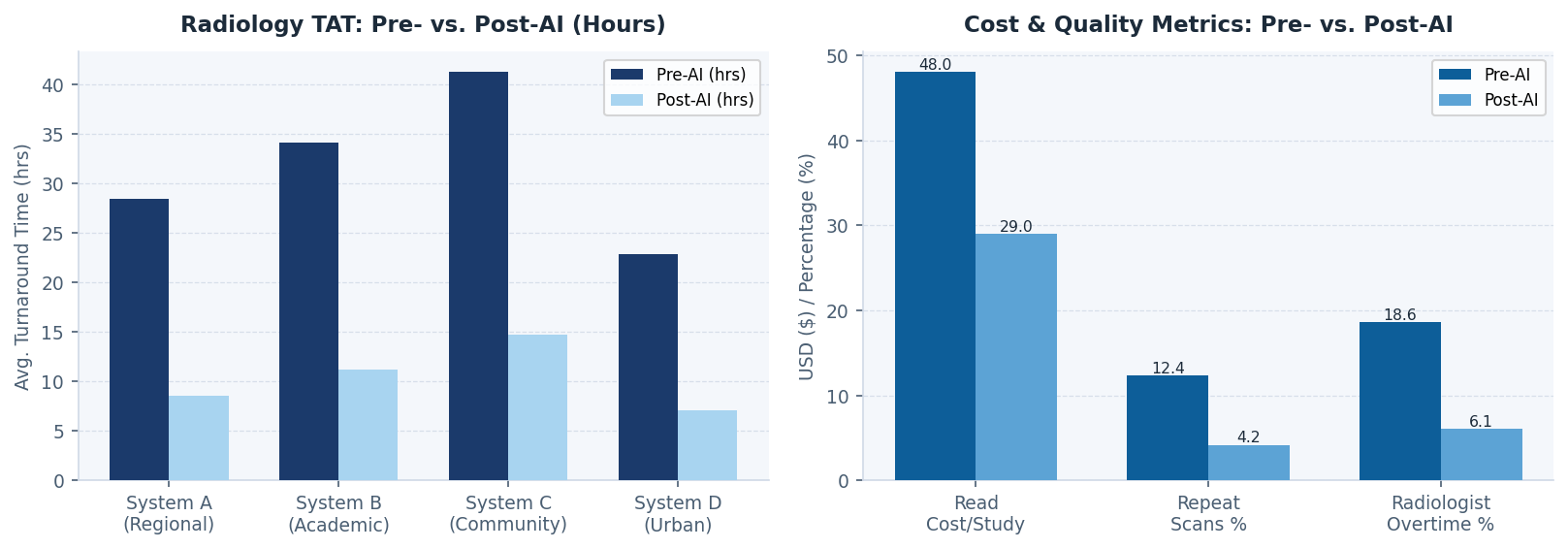
Figure 2 — Radiology Turnaround Time & Cost/Quality Metrics: Pre- vs. Post-AI Deployment
Building the 12-Month Payback Model
A credible payback analysis for a hospital system considering a radiology AI investment should model four categories of benefit: read capacity uplift (how many additional studies can be processed without incremental radiologist FTEs), cost-per-study reduction, repeat scan elimination, and overtime normalisation.
For a 500-bed system performing 300,000 imaging studies annually, these four levers typically generate combined Year 1 financial benefit in the range of $8–14 million. Implementation costs — including platform licensing, integration with the PACS and RIS, staff training, and model validation — typically run $4–6 million for a system of this scale. The 12-month payback case is achievable, but it requires rigorous baseline measurement and a program that addresses all four benefit levers, not just throughput.
The systems that achieve payback on schedule share a common characteristic: their radiology and finance leadership treated this as a joint program from the start. Radiology provides the clinical expertise to validate AI output and manage the exception queue. Finance provides the measurement framework to capture the savings. When those two functions are aligned from day one, the implementation stays on track and the business case stays honest.
Beyond the Payback Period
The financial case for radiology AI does not peak at month 12. As AI models improve on each institution's specific scanner hardware and patient population, accuracy increases and the exception queue — studies requiring additional human review — shrinks further. Systems that have been running AI-assisted reading for 24–36 months report continued improvement in both throughput and diagnostic confidence metrics.
The longer-term strategic value is in what radiology departments can do with the capacity they recover. Sub-speciality reads that were previously outsourced due to internal capacity constraints can be brought in-house. Teleradiology costs decline. Radiologists shift from volume reading toward complex case consultation and AI model oversight — work that commands higher reimbursement and carries better retention economics. The 12-month payback is the beginning of the financial story, not the end of it.
Comments (0)
Join the conversation!